
It's Monday morning rounds at a Dubai hospital. You're seeing a 52-year-old Emirati patient with chest discomfort — could be anxiety, reflux, or angina. The conversation switches between Arabic and English. You're mentally running through the differential while trying to remember what to document, which tests to order, and whether you asked about family history.
By the time you finish typing the note 15 minutes later, you've forgotten two important details you meant to include.
This scenario plays out daily across GCC hospitals. While AI medical scribes have solved documentation burden, a critical gap remains.
This Guide Will Show You
- What AI medical scribes solve (and what they miss)
- Why in-consultation diagnostic assistance is the next evolution
- What to look for in platforms combining both capabilities
- How this technology is being implemented in GCC healthcare
If you're using ambient documentation but still worried about diagnostic uncertainty — this is for you.
What Is an AI Medical Scribe?
An AI medical scribe listens to doctor-patient conversations and automatically generates clinical documentation — converting natural conversation into structured SOAP notes, H&Ps, or progress notes.
How they work: Capture audio → transcribe conversation → apply NLP to structure content → generate draft note for review.
In GCC: Ambient scribes are now deployed across major UAE and Saudi hospitals. The technology has matured significantly, with advanced platforms handling multilingual consultations (Arabic + English code-switching) effectively.
Clinicians using ambient documentation save 60–90 minutes daily on note-writing.
What Ambient Documentation Has Solved
AI medical scribes have delivered measurable wins across the region:
- Time Reclaimed. Physicians report finishing documentation within minutes instead of hours — 60–90 minutes back daily for patient care or personal time.
- Multilingual Capability. Newer platforms handle seamless Arabic-English code-switching effectively, addressing a critical GCC requirement that early scribes couldn't meet.
- Reduced Burnout. Clinicians across the Emirates report 70%+ reduction in after-hours documentation time. No more staying late to finish charts.
- Better Patient Presence. Without a laptop barrier during consultations, physicians maintain eye contact and are fully present. Patients notice the difference.
Documentation efficiency is now a solved problem for clinics that have adopted ambient listening.
The Gap That Documentation Alone Can't Fill
- Diagnostic Uncertainty. You're seeing vague abdominal pain. Is this IBS? Appendicitis? Ectopic pregnancy? Your scribe documents whatever you conclude — it doesn't help you systematically work through the differential.
- Missed Critical Context. The patient mentions their father died suddenly at 50 from an MI, but the detail doesn't register as a red flag. The scribe captures what was said but doesn't flag familial cardiovascular risk.
- Evidence Gaps at Point of Care. You know there's a NICE guideline or local protocol but can't recall specifics. Your scribe writes what you prescribed — it doesn't retrieve evidence during the consultation.
- Fragmented Patient History. The patient saw cardiology at Sheikh Khalifa, has labs from Cleveland Clinic Abu Dhabi, takes medications from three pharmacies. A scribe documents this visit — it doesn't synthesize the complete story.
- Red Flag Blindness. During a busy clinic, the patient mentions worsening headaches with neck pain, but you're juggling five things. The note documents "headache" — it won't alert you that this combination needs urgent imaging.
Faster documentation is essential. But documentation alone doesn't reduce diagnostic errors.
Enter: In-Consultation Diagnostic Assistants
The healthcare AI market is evolving beyond transcription to actively support diagnostic reasoning during encounters.
The fundamental difference: While ambient scribes optimize documentation of clinical thinking, diagnostic assistants actively support clinical thinking in real-time.
Core capabilities in this emerging category:
- Real-time differential diagnosis generation
- Evidence-linked recommendations with citations
- Automatic patient context retrieval from EHR
- Red flag and critical finding detection
- Structured clinical reasoning workspace
The clinical need is substantial. Diagnostic errors affect an estimated 1 in 20 patients globally. Unlike documentation efficiency — where the problem was clear — diagnostic safety requires fundamentally different technical and clinical approaches.
How In-Consultation Diagnostic Assistance Works
The most sophisticated implementations combine four core capabilities:
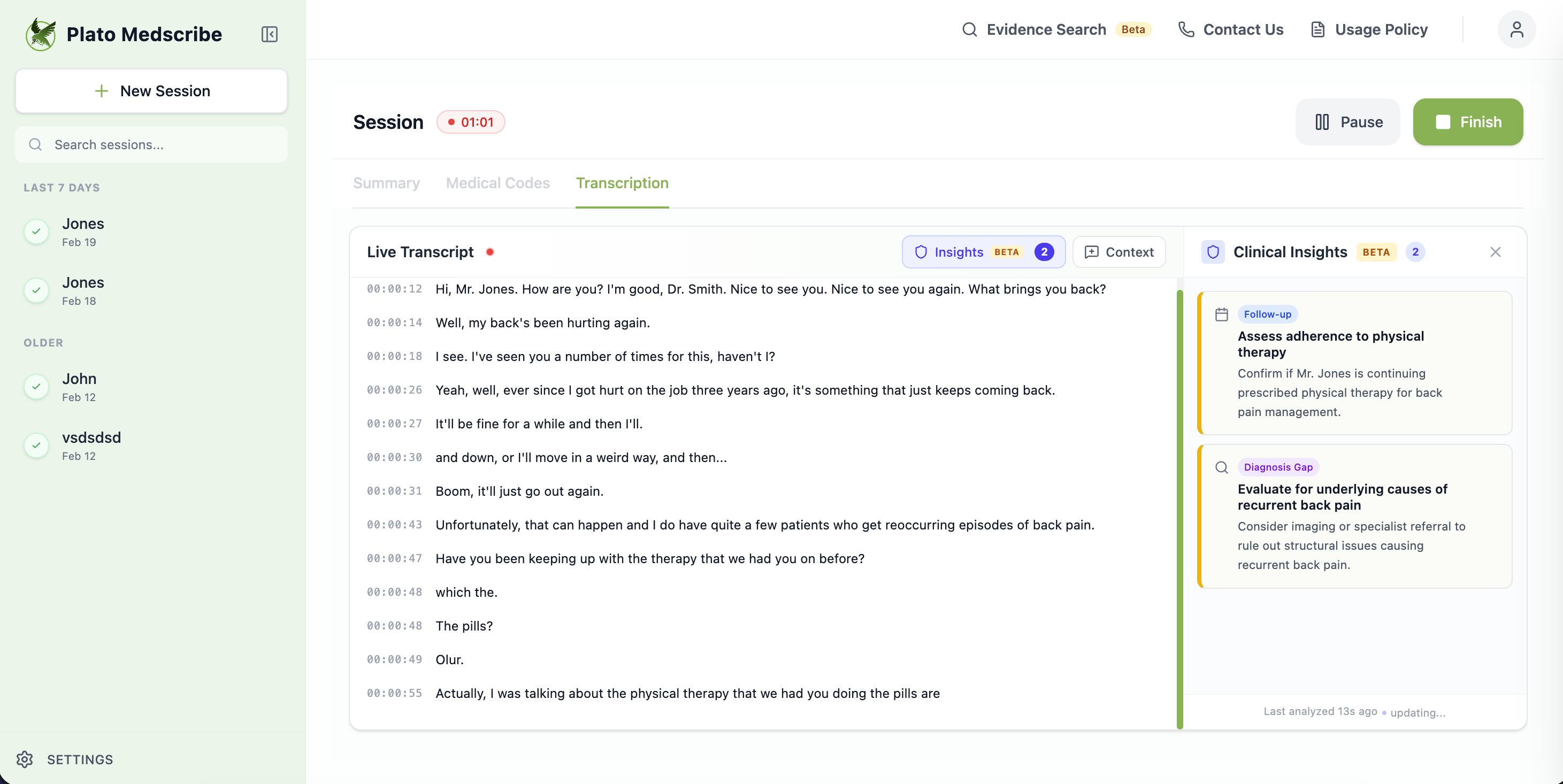
1. Real-Time Structured Clinical Thinking
Rather than just transcribing, the system builds a structured clinical workspace during conversation:
- Presenting symptoms organized by system
- Timeline and duration clearly mapped
- Red flags automatically highlighted
- Relevant positives and negatives tracked
- Medications, allergies, and risk factors surfaced
The value: An organized problem representation during the encounter — when you can still ask follow-up questions.
2. Evidence-Linked Differential Suggestions
This is the most technically and clinically complex capability. Based on the conversation and structured facts, the system suggests possible diagnoses — but critically, never as autonomous decisions.
Well-designed systems include:
- Clinical reasoning. Why this diagnosis is being considered.
- Supporting findings. Which specific patient details triggered this suggestion.
- Evidence citations. Guidelines from NICE, local hospital protocols, or international standards.
- Confidence levels. Explicit uncertainty communication.
- Reviewable basis. Transparent reasoning you can verify independently.
Example clinical scenario: 45-year-old presenting with chest discomfort, dyspnea, recent long-haul flight from London to Dubai.
What a diagnostic assistant might surface:
- Consider PE given recent prolonged travel (Wells score calculation suggested)
- Evidence: NICE guidance NG158 on VTE diagnosis
- Next steps: D-dimer if low/moderate probability, CTPA if high probability
- Safety note: Rule out life-threatening causes before attributing to anxiety
The critical design principle: You must be able to independently review the basis for recommendations. This aligns with FDA clinical decision support guidance emphasizing clinicians should not rely primarily on software outputs.
3. One-Click Patient Context Integration
The best implementations automatically retrieve relevant patient information when launched:
- Current medications and allergies
- Active problem list and chronic conditions
- Recent labs and imaging with findings
- Specialist visit notes from recent months
- Overdue screenings and care gaps
All with timestamps and source attribution for provenance verification.
GCC relevance: Patients often receive care across multiple facilities (Mediclinic, Saudi German Hospitals, SEHA). Automated context retrieval helps clinicians see the complete picture quickly.
Technical requirement: Most systems use SMART on FHIR for EHR integration.
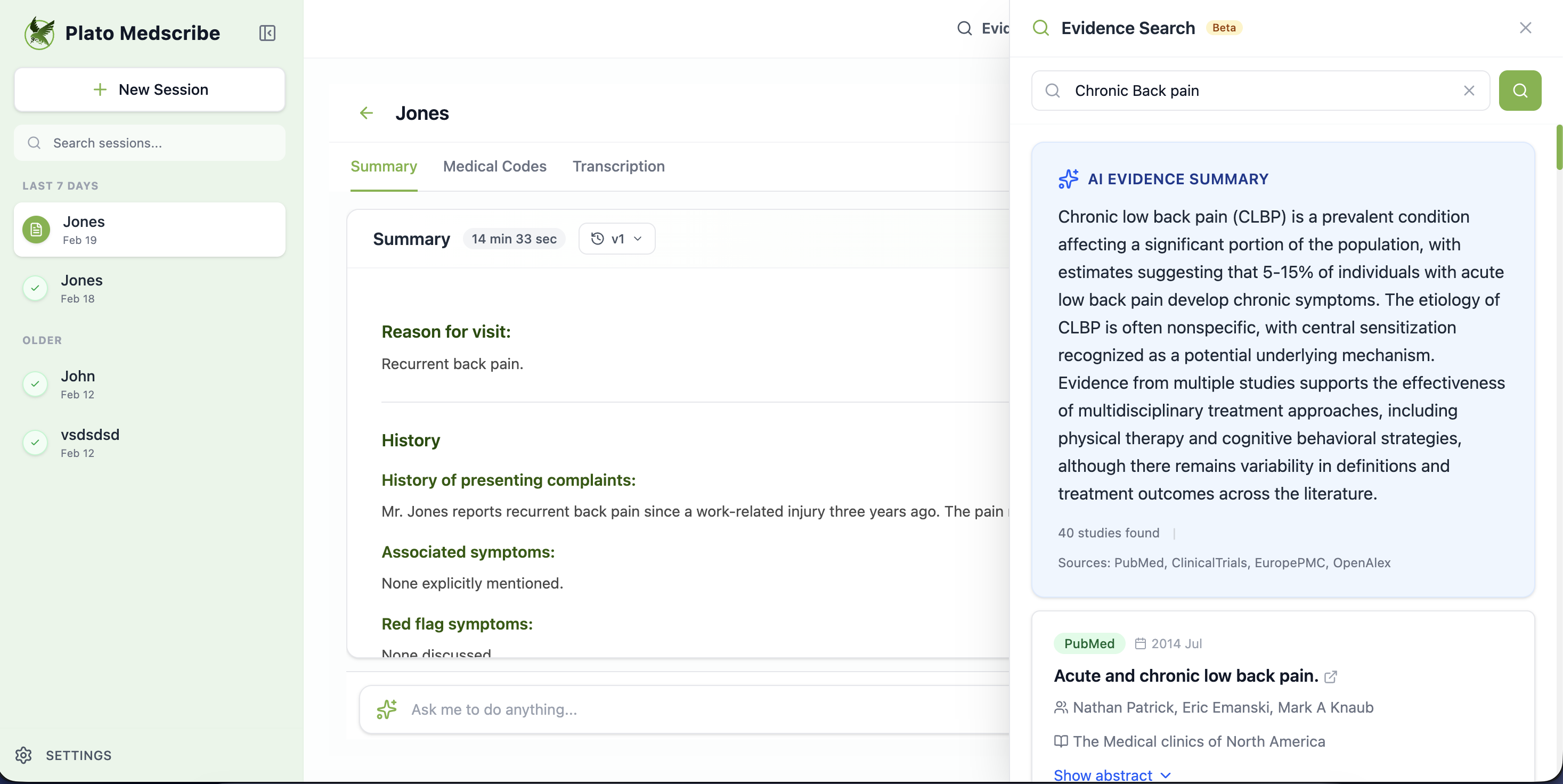
4. Searchable Clinical Knowledge Base
During consultations, clinicians can ask clinical questions directly:
- "What's first-line for new-onset AFib in this patient?"
- "Does diabetes change antibiotic choice for UTI?"
Quality implementations provide:
- Citations to underlying guidelines or studies
- Version dates ensuring currency
- Contraindications and special considerations
- Local formulary preferences where configured
GCC customization: Systems can be configured with local hospital protocols (UAE hospital policies, SEHA guidelines, MOH Saudi standards) and regional antimicrobial stewardship preferences.
Why Integration Matters: The Combined Approach
When ambient listening and diagnostic assistance share the same conversation stream, diagnostic suggestions are based on exactly what was discussed — not what you manually typed into a search box.
The flywheel effect: Better transcription → accurate problem representation → relevant differential suggestions → less time searching → more time with patient.
The evolution:
- Generation 1: Manual documentation (slow, exhausting)
- Generation 2: Ambient scribes (fast documentation)
- Generation 3: Ambient + diagnostic intelligence (documentation + safer decisions)
Comparing Clinical Documentation Approaches
Let's compare the main approaches without vendor bias:
| Capability | Manual Documentation | Traditional AI Scribe | Diagnostic Assistant Platform |
|---|---|---|---|
| Generates clinical notes | ❌ Manual typing | ✅ Automatic | ✅ Automatic |
| Time savings | Baseline (slowest) | ✅ 60–90 min/day | ✅ 60–90 min/day |
| Handles Arabic + English | ✅ If you speak both | ⚠️ Limited | ✅ Advanced platforms |
| Real-time differential diagnosis | ❌ Mental only | ❌ Not included | ✅ Evidence-linked |
| Patient context from EHR | ❌ Manual search | ❌ Documents what you know | ✅ Automatic retrieval |
| Evidence-based recommendations | ❌ Separate search | ❌ Not included | ✅ With citations |
| Red flag detection | ❌ Clinician must catch | ❌ Documents only | ✅ Automated highlighting |
| Primary value | None (baseline) | Administrative efficiency | Efficiency + Diagnostic safety |
Key insight: Traditional AI scribes solve documentation burden. Diagnostic assistant platforms address both documentation efficiency and diagnostic safety — the complete solution for GCC clinicians managing complex multilingual consultations with diagnostic uncertainty.
Evaluating Solutions: What Actually Matters
✓ What Matters
- Transparent Reasoning. Can you see which patient findings and evidence sources led to each suggestion? Black-box recommendations create liability risk.
- Avoids Alert Fatigue. Traditional CDS systems have 90%+ override rates. Look for pull-based suggestions at natural decision points, not interruptive pop-ups.
- Evidence Citations. Every clinical claim should cite source guidelines with publication dates and versions.
- Regional Support. For GCC deployment, platforms must handle Arabic medical terminology, language switching, local protocols (SEHA, MOH Saudi), and regional compliance (SDAIA, UAE Data Office).
- EHR Integration. SMART on FHIR for seamless patient context passing from major systems (Epic, Cerner, Meditech).
- Safety Governance. Look for tracking of acceptance rates, safety incident reviews, and continuous improvement analytics.
The Regulatory Reality
- United States. FDA guidance states CDS outputs must enable clinicians to independently review the basis for recommendations — systems must show their reasoning transparently.
- European Union. MDR generally classifies decision support software combining medical knowledge with patient data as medical devices (Class IIa/IIb/III).
- GCC. SDAIA (Saudi Arabia) and UAE Data Office have specific requirements for healthcare AI. When evaluating vendors, understand their regulatory posture and compliance documentation.
Implementation Considerations for GCC Healthcare
- Starting safely. Pilot with 3–5 clinicians in lower-risk settings before broader deployment. Measure acceptance rates, workflow impact, and safety concerns over 2–4 weeks.
- Integration. Understand your IT environment's readiness. SMART on FHIR is standard but requires EHR vendor support. Some facilities start with standalone overlays before deeper integration.
- Change management. Even passive assistance changes workflow. Transparency about how recommendations are generated helps build clinician trust.
- Compliance. Ensure clarity about data processing location, encryption, retention policies, and alignment with SDAIA/UAE Data Office requirements.
Common Questions
Don't diagnostic assistants slow down consultations?
Done poorly, yes. Done well, no. The key is pull-based interaction — you access suggestions when ready, not via interruptive pop-ups.
How accurate are AI diagnostic suggestions?
Responsible platforms communicate uncertainty explicitly, provide evidence for review, and undergo clinical validation. Always ask vendors: "Where's the clinical evidence?"
What about patient privacy?
Look for clear consent workflows, HIPAA and GDPR compliance, data residency guarantees, encryption, and configurable retention policies aligned with SDAIA/UAE Data Office requirements.
Can these integrate with our EHR?
Most modern platforms support SMART on FHIR for launching with patient context automatically loaded. Integration depth varies by vendor and IT environment.
How do we pilot safely?
Start with 3–5 clinicians in lower-acuity settings for 2–4 weeks. Measure acceptance rates, time impact, and safety concerns before broader deployment.
The Path Forward: Documentation + Diagnostic Intelligence
Ambient scribes proved in-room listening works at scale. The next evolution uses that capability to improve both efficiency and diagnostic safety.
The opportunity in GCC:
- Diagnostic uncertainty affects busy clinics
- Multilingual consultations add complexity
- Regional protocols require customization
- Clinicians want support but reject poorly-designed alerts
What's emerging: Platforms combining proven ambient documentation with evidence-based diagnostic assistance — both working together during consultations on integrated systems.
The goal: augment clinical judgment at the moment it matters most — when you can still ask the next question or order the right test.
Plato: Combining Ambient Documentation with Diagnostic Intelligence
Plato has been deployed across GCC hospitals for ambient clinical documentation, with physicians reporting 60–90 minute daily time savings. The platform handles Arabic-English code-switching effectively.
Now available: Plato MedAssist
Building on proven ambient listening, Plato MedAssist adds the diagnostic intelligence layer:
- Real-time differential suggestions with evidence citations
- Automatic patient context retrieval from EHR
- Searchable clinical knowledge base with local UAE/Saudi guidelines
- Red flag detection and structured reasoning workspace
- SDAIA certified and UAE Data Office compliant
Plato is the first platform in the GCC to offer both ambient documentation and in-consultation diagnostic assistance in one integrated solution.
See Both Capabilities Working Together
For existing Plato users, MedAssist enhances your current workflow without disrupting it. For new evaluations, see ambient documentation and diagnostic intelligence on one platform.
Request a Demo →


